
Review Article | DOI: https://doi.org/10.31579/2578-8868/149
Department of Medicine, University of the Region of Joinville, Rua Ministro Calógeras, 439, Bucarein, Joinville, Santa Catarina, Brazil,
*Corresponding Author: Marco Antônio Machado Schlindwein, Department of Medicine, University of the Region of Joinville, Rua Ministro Calógeras, 439, Bucarein, Joinville, Santa Catarina, Brazil,
Citation: Machado Schlindwein MA., Isabelle P. Bandeira., Letícia C. Breis., Guilherme S. Mendonça., Marcus V. Magno Gonçalves.,. (2021) Anti-CASPR2 and Epilepsy: don’t forget to think about it. J. Neuroscience and Neurological Surgery. 8(2); DOI:10.31579/2578-8868/149
Copyright: © 2021 Marco Antônio Machado Schlindwein, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 11 January 2021 | Accepted: 11 April 2021 | Published: 23 April 2021
Keywords: CASPR2; epilepsy; autoimmune encephalitis; autoimmune epilepsy
Autoimmune encephalitis (AE) is an important cause of seizures. With the discovery of highly specific neuronal-antibodies the recognition of the clinical syndrome associated with each marker is crucial to the right diagnosis and treatment regime. In this short review we summarize the importance of CASPR2 antibodies in unknown etiology seizures and its epileptogenesis.
Autoimmune encephalitis (AE) is a growing field in neurology. The discovery of highly specific neuronal-antibodie [1] makes a typical syndrome recognition important to reach the correct antibody diagnosis and correct treatment regimen important. Thus, it is possible to achieve the correct diagnosis of these antibodies and the eligible treatment regimen.
Seizures are a common presentation among those with AEs, with 20% of them being diagnosed with epilepsy on admission [2]. It is interesting to note that the cluster of evidence involving neuronal antibodies and epilepsy is still growing. In a study evaluating the prevalence of these antibodies in patients with new and/or established epilepsy, It was found that 11% of those had positive antibodies with antibodies against Voltage-Gated potassium channel (VGKC) complex , representing almost half of them [3]. A similar result occurs in a study that evaluated children with new-onset seizures, of which 9.7% had positive antineuronal antibodies with CASPR2 (the second more frequently found) [4]. In the pediatric cohort of Wright et al. (2016) the results were very similar [5].
Contactin-associated protein-like 2 (CASPR2) is a cell adhesion molecule with an important function in clustering VGKC in the juxtaparanodal region of the Node of Ranvier [6]. Together with Leucine-Rich Glioma-Inactivated 1 (LGI-1) protein, CASPR2 (anti-CASPR2) antibodies form among patients who have VGKC antibodies [7]. Although seizures appear more frequently in anti-LGI-1 (80%) patients than in patients positive for anti-CASPR2 (49%) [8,9] other studies have actually shown that seizure is also a common symptom in CASPR2 antibodies disease in children [10] and in adults 8,10,11 The incidence of positive antibody patients can reach up to half of the patients [8].
Curiously, the prevalence of neuronal antibodies appears to be higher in some subtypes of epileptic syndromes [4,12,13]. Ekizoglu and colleagues evaluated the prevalence of neuronal antibodies in patients with focal-epilepsy of unknown cause and mesial temporal lobe epilepsy with hippocampal sclerosis: 16% of patients were positive for neuronal antibodies, with 4.9% of patients positive for CASPR2 specifically [12]. In temporal lobe epilepsy, the prevalence found was 5%, with antibodies. Of these, 4 patients were positive for CASPR2 [14]. Afterward, in a cohort study that included patients with late-onset epilepsy, CASPR2 was the only specific neuronal antibody found (3%) [15].
Therefore, temporal lobe epilepsy with or without hippocampus atrophy, focal epilepsy of unknown origin, epilepsy with peri-ictal autonomic disturbance and late-onset epilepsy may place anti-CASPR2 encephalitis on the differential diagnosis table [12-15]. Epileptic activity on the initial electroencephalogram (EEG) appeared only in 30% of patients with CASPR2 [8]. Consequently, it is extremely important to pay attention to clinical details that can help clarify the diagnosis.
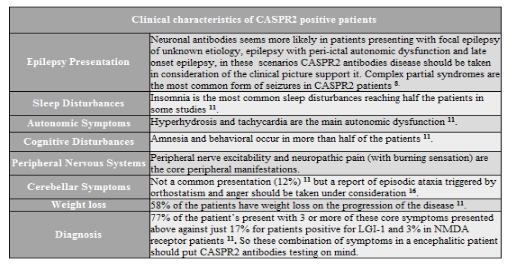
Among those details, we highlight: patients with advanced age, presenting with a sub-acute progressive cognitive decline, or sleep disorders, as well as psychiatric complaints of recent onset, autonomic dysfunction (especially hyperhidrosis and heart rhythm abnormalities). Other red flags may be cerebellar symptoms and impairment of the peripheral nervous system, especially neuropathic pain and neuromyotonia (Table 1) [8,10,11,16]. These data advise in favor of disease with positive CASPR2 antibodies.
In addition, a worrying fact in anti-CASPR2 encephalitis is that a great amount of the patients do not present changes in the magnetic resonance image; the image is normal, without registering T2 hyper-intensities [8,10,11] especially in the initial presentation [8]. That is why normal imaging does not exclude AE, including anti-CASPR2 encephalitis.
These findings are probably related to the fact that CASPR2 antibodies are of the IgG4 subclass and do not activate complement, nor do they induce internalization (common features in other AE syndromes). On the other hand, disrupt the interaction between CASPR2 and transient axonal glycoprotein-1 (TAG-1) where they make the clustering of the juxtaparanode VGKC [17-19]
However, the distribution of VGKC along the axon relies on this interaction (CASPR2 and TAG-1) especially in the juxtaparanodal region, which are important for the control of neural excitability [20].
The epileptogenesis activity linked to anti-CASPR2 antibodies is not completely defined, although there is evidence that these antibodies target the inhibitory neurons in the hippocampus [21] causing an increase in the VGKC and reducing the activity of these neuronal cells [19]. It is believed that this cascade of phenomena results in an increase in the triggering activity of the CA3 neurons in the hippocampus, giving rise to the seizure crisis [22]. Also, functional neuroimagem studies have already reported abnormalities in the hippocampus associated with anti-CASPR2 patients [23], whilst this has been correlated with amnesia and not with epileptic activity itself.
In conclusion, CASPR2 antibodies often present with seizures, and the primary diagnosis for these patients may be epilepsy. Therefore, a carefully clinical evaluation can help guide the screening of antibodies and the establishment of the correct treatment. Finally, further studies are needed to elucidate the pathogenesis of epilepsy associated with anti-CASPR2, and thus complement the puzzle of Unknown Etiology Seizures
Disclosure of conflict of interest
None of the authors has any conflict of interest to disclose.
Ethical Publication Statement
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
